Sleep Diagnostics · New Service
The problem: when a "normal" sleep study isn't normal
A familiar scene in clinic. Someone in their thirties or forties comes in exhausted. They wake up unrefreshed, they fall asleep in meetings, their partner says they sometimes pause their breathing — but the home sleep study comes back with an AHI of 3 and a clean bill of health. They are told there is nothing wrong. They keep feeling terrible.
The same scene happens a different way. Someone on CPAP. Their residual AHI is 0.2. The machine reports a perfect night. They still feel awful and CPAP hasn't made them feel any better.
Both of these patterns are consistent with Upper Airway Resistance Syndrome (UARS) — and standard sleep studies are not built to find it.
What UARS actually is
Snoring and sleep apnoea sit at two ends of a spectrum. At one end, the airway vibrates but stays mostly open. At the other, it closes completely, oxygen falls, and the brain wakes you up to start breathing again. UARS sits somewhere in between — but mechanically it is its own thing.
In UARS, the airway is so narrow during sleep that the patient is working extremely hard to move air through it. They are not stopping breathing. They are not desaturating. They may not even be obviously arousing. But the muscular effort of breathing is enormous, sustained over hours, every night. By morning the body has effectively been doing a workout for eight hours. That is why these patients wake exhausted.
The condition was first defined by Christian Guilleminault at Stanford. The diagnostic gold standard he proposed was oesophageal manometry: a thin pressure catheter passed through the nose into the oesophagus, sitting at chest level overnight, directly measuring the swings in intrathoracic pressure that signal respiratory effort. It works — but only about 80% of patients can tolerate it, and the catheter itself partially splints the airway open, blunting the very signal it is trying to measure. It is also unavailable in most sleep labs.
What Michael and I have been building
The question we set ourselves: can we get the same information non-invasively, from a standard home sleep study, without a tube in the nose?
The answer is yes — if you stop relying on apnoeas and oxygen drops and start looking at respiratory effort itself. We have built an analysis suite that pulls four categories of marker out of a routine polysomnogram or home sleep study:
- RDI (Respiratory Disturbance Index) — the standard sum of apnoeas, hypopnoeas and respiratory-effort-related arousals (RERAs). Useful but blunt.
- RERAs and flow limitation — extracted from the nasal pressure trace, more sensitive than AHI alone. Good when the nose is clear; less reliable in patients with nasal blockage.
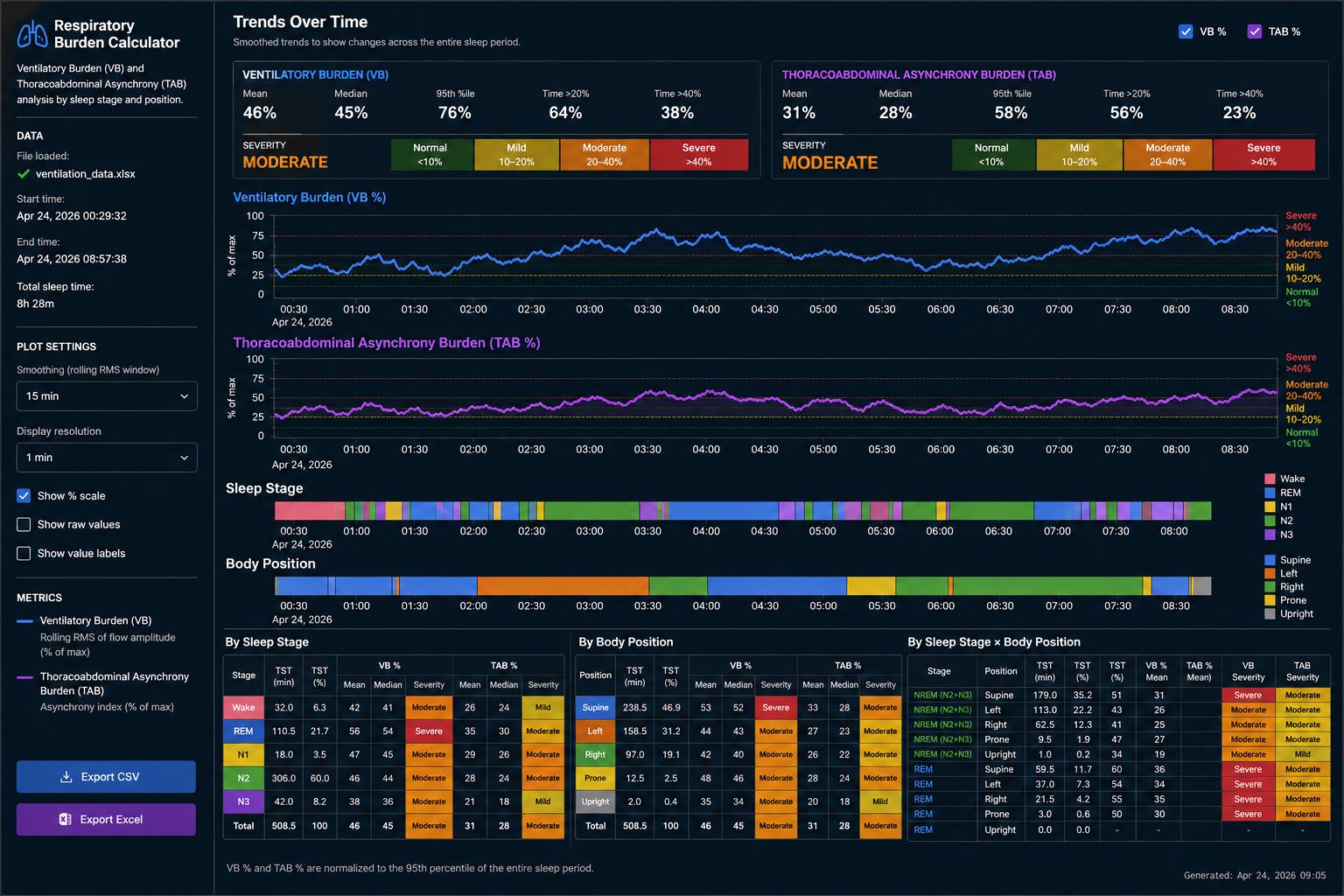
- Ventilatory Burden (VB) — a marker NOX Medical are bringing out shortly. We have implemented our own version. It measures, across the night, what percentage of breaths fall below an individualised baseline of inspiratory flow.
- Thoracoabdominal Asynchrony Burden (TAB) — our own metric, extracted from the sleep study parameters that show chest and abdominal effort without relying on arousals. When you are struggling to breathe, the chest and abdomen have to work harder to overcome that obstruction or resistance. TAB gives us a clear number about how much effort the body is making just to keep breathing. To improve accuracy we also break it down by sleep stage and by body position.
- Autonomic Burden (AB) — our newest metric, and the one we are most excited about. AB measures how much sympathetic ("fight-or-flight") nervous-system drive the body is experiencing during sleep, using markers such as heart-rate variability, pulse-rate response and peripheral autonomic signals. In simple terms, it shows how stressed the body is overnight, even when the patient appears to be sleeping calmly. AB is calculated from three consecutive nights of Nox T3s sleep-study data so we can see the patient's true baseline rather than a single-night snapshot. It is a new value we have developed in-house and it is already working very well for our patients.
Bringing the three burdens together — VB, TAB & AB
Each of these metrics tells a different part of the story:
- VB is about airflow — how unstable or impaired the ventilation itself was.
- TAB is about effort — how hard the chest and abdomen were working.
- AB is about physiological cost — how much sympathetic stress the body absorbed as a result.
Looked at on its own, any one of these can mislead. Looked at together, they let us separate genuinely distinct sleep phenotypes that the standard AHI lumps into one bucket — and, crucially, they explain why two patients with the same AHI can feel completely differently in the morning.
How the combinations help — in plain English
A few of the patterns we use most often in clinic:
- High VB + High TAB + High AB. The body is unstable on every axis — disturbed airflow, heavy respiratory effort, and a large autonomic price being paid. This is classic significant sleep-disordered breathing, often with UARS-like or even sleep apnoea physiology, and the patient typically feels terrible despite whatever the AHI says.
- Low VB + High TAB + High AB. The airflow looks reasonable, but the chest and abdomen are fighting hard and the autonomic system is paying for it. This is the "silent UARS" pattern — the patient is working extremely hard to breathe yet not desaturating or arousing, and the conventional study reports them as normal. They are exactly the patients we built this service to find.
- Low VB + Low TAB + High AB. The respiratory mechanics look fine, but the body is still in sympathetic overdrive at night. This often points to a low arousal threshold, autonomic instability, insomnia-related physiology, or very subtle flow limitation that VB and TAB are not capturing on their own. It also flags patients whose tiredness is autonomic rather than purely respiratory.
- Low VB with other changes in TAB and AB. Using other combinations of our new metrics we have found that so useful in understanding why some patients are not improving with certain treatments. For example some patients on CPAP have a completely normal AHI (sometimes 0.1), but they still feel just as tired in the morning. Using TAB and AB we have found that we can work out if the CPAP is just not working hard enough or working too hard and pushing back on the patient's ability to breathe too much. We are seeing how it can help patients who have a mandibular advancement device (mouth gaurd), and show when teeth grinding (bruxism) might be an attempt by the body to try and keep the airway open. We are looking into the effect of Restless Leg Syndrome or Periodic Limb Movememnt Disorder might be affecting our breathing at night and how we feel in the morning.
Why this is so useful for CPAP patients who still feel tired
One of the most rewarding uses of the three-burden framework is in patients already on CPAP, BiPAP or a mandibular device, whose residual AHI looks excellent but who still wake up exhausted. The combined VB / TAB / AB pattern usually tells us which of two things is happening:
- The pressure is too low. VB and TAB stay elevated, AB stays high — the airway is still narrowing and the body is still paying the autonomic cost. The machine is recording "no apnoeas" but the patient is functioning as if untreated.
- The pressure is too high. VB and TAB look clean, but AB is high. The patient is being "inflated" beyond what their respiratory drive wants, central events and arousals creep in, and the sympathetic system stays switched on. They wake up unrested for the opposite reason.
Either way, the three-burden read-out points directly at why the patient is not feeling better, and gives us a rational starting point for adjusting the therapy.
Why three nights of Nox T3s data?
Single-night sleep studies are very noisy — especially for the autonomic signal, which is sensitive to a bad day, a glass of wine, anxiety about the device on the chest, or a poor sleep position by chance. We use three consecutive nights of recording on the Nox T3s home sleep-study device so that we can see what the patient's body is genuinely doing during sleep rather than what it did on one unrepresentative night. There is significant night-to-night variability that changes the AHI considerably - The AB calculation in particular needs this three-night window to be reliable.
These three burdens — VB, TAB and AB — are new values that we have developed into our own work, not yet part of international consensus criteria. They are working very well for our patients in real clinical use, and they routinely identify problems that standard sleep-study reporting misses.
Why TAB matters
The crucial group of UARS patients are the ones who are not waking up. They have low RERAs because their cortical arousal threshold has adapted — their brain has learned to keep them asleep despite the effort. If you look at their sleep study with the standard arousal-based markers, the report looks fine. But their respiratory effort is enormous.
TAB captures that effort directly. It does not need an arousal. It does not need a desaturation. It just needs the chest and the abdomen to be doing the work of breathing slightly out of sync — which they reliably are when the airway is narrow. This is the marker that Christian Guilleminault needed, but he had to use oesophageal manometry instead
That is the group we think the TAB score will help most: patients with what we would informally call "silent UARS" — debilitating tiredness, a clean conventional study, and no obvious explanation.
Who this service is for
- Patients with daytime fatigue and a "normal" home sleep study or polysomnogram
- Patients on CPAP, a mandibular advancement device, or post-surgery with a low residual AHI but persistent unrefreshing sleep
- Patients who feel their wearable or sleep-tracker data shows something the formal report missed
- Clinicians who would like a TAB / VB re-analysis of an existing study they have done elsewhere
- Patients enrolled in the wider MDT Sleep Programme or considering surgical assessment
How the service works
- Existing study, or new one. Bring an existing home study or polysomnogram for re-analysis, or arrange a new three-night Nox T3s home sleep study via courier through the practice. Three consective nights is the minimum needed for the AB calculation to be reliable.
- Full VB, TAB & AB analysis. Michael and his team run the recording through our new scoring engine to produce per-stage and per-position Ventilatory Burden, Thoracoabdominal Asynchrony Burden and Autonomic Burden, alongside the standard RDI, RERA and flow-limitation markers.
- Clinical interpretation. Professor Veer reviews the results in the context of your symptoms, anatomy and any prior treatment.
- Plan. Where UARS is identified, treatment options are discussed within the same framework as conventional OSA — positional therapy, nasal optimisation, mandibular devices, CPAP at lower pressures, or surgical assessment via DISE or the MDT.
Important caveats
This is a new analysis service developed by Professor Veer and Michael Storey. The metrics are not yet incorporated into international consensus guidelines, and the information we are gathering will be part of a medical research study that we creating. The results inform but do not replace overall clinical judgement.
If you have severe daytime sleepiness, recent loss of consciousness, or symptoms suggestive of significant sleep apnoea, please arrange a formal sleep assessment urgently rather than waiting for a specialist re-analysis.
Get in touch
To enquire about a TAB / VB analysis — whether of an existing study you already have, or a fresh home sleep study — contact my secretary.