What Is Drug Induced Sleep Endoscopy?
Drug Induced Sleep Endoscopy — DISE — is a short diagnostic procedure in which a carefully controlled amount of anaesthetic is given to replicate a sleep-like state. At the same time, a thin flexible camera (nasendoscope) is passed gently through the nose to examine the throat while the patient is asleep. Because the patient is genuinely unconscious and breathing spontaneously, the tissues of the throat relax and obstruct in the same way they do at night — making it possible to see precisely where, and how, the airway collapses.
DISE was first described by Croft and Pringle in 1991 — at the Royal National Throat Nose and Ear Hospital, the same institution where Professor Veer leads the sleep surgery programme today. In the three decades since, it has become one of the most widely used diagnostic investigations in sleep surgery worldwide, offering something no other technique can provide: a dynamic endoscopic view of the airway during actual (or simulated) sleep.
It is currently the only clinically acceptable way of obtaining a dynamic endoscopic examination of upper airway obstruction during a state that replicates natural sleep. Static imaging (CT, MRI), awake endoscopy, or sleep study data alone cannot tell you which specific anatomical structures are collapsing, or in what combination — but DISE can.
"After years of suffering from suspected sleep apnoea, I came across Mr Vik Veer's in-depth YouTube videos on the topic. For the first time I felt that someone really understood the issues I'd been having and would do their utmost to find the right solutions going forward." Google Review, 5 stars — Chris Ade
Why DISE Is Central to Surgical Planning
Obstructive sleep apnoea is not one condition. It is the result of one or more specific structures collapsing in one or more locations in the throat during sleep. The palate, the tonsils, the lateral pharyngeal walls, the tongue base, and the epiglottis can all contribute — independently or together — and the combination is different in every patient.
This matters enormously for surgery. A surgeon who operates only on the palate will cure the patient who has purely palatal obstruction — and do essentially nothing for the patient whose airway collapses at the tongue base or epiglottis. In the early days of sleep surgery, operations were often chosen based on anatomy visible in the clinic — tonsil size, palate position, tongue position — rather than on what actually happened during sleep. Results were unpredictable. Some patients improved dramatically; others did not benefit at all from the same operation.
DISE changed this. With a genuine dynamic view of the sleeping airway, a surgeon can see that this patient has palatal flutter and tongue base collapse, but intact lateral walls; that patient has bilateral lateral wall collapse requiring pharyngoplasty; another has a trapdoor epiglottis — a finding invisible on any other examination — which is actually the dominant obstruction and explains why CPAP was making things worse. These distinctions dictate entirely different surgical plans, and DISE is the only investigation that reveals them.
The Problem With DISE: Classification
Despite its obvious diagnostic value, DISE was for many years hampered by a fundamental problem: no agreed way to record or communicate what was seen. Dozens of classification systems were proposed — VOTE, NOHL, Croft and Pringle, DISE Index, and many others — but none achieved widespread adoption, and inter-rater reliability between surgeons using different systems was poor.
This had practical and research consequences. In a busy sleep surgery centre, two surgeons examining the same patient might record different findings and propose different operations. In multicentre research, DISE findings from different centres were effectively incomparable. And for trainees, the learning curve was steep — experienced surgeons could identify subtle patterns that junior colleagues missed entirely.
Professor Veer began investigating this problem in 2014, conducting qualitative semi-structured interviews with ENT trainees immediately after DISE procedures to understand exactly where and why classification systems were failing them.
Professor Veer's Modified DISE Technique
Before addressing the classification, there is a more fundamental question about DISE itself: is the anaesthetic state it produces a faithful representation of sleep? Propofol — the drug used in the vast majority of DISE procedures worldwide — creates a state of anaesthesia, not sleep. The two are not the same thing.
Under conventional target-controlled infusion (TCI) propofol, respiration is typically regular, muscle tone is uniformly suppressed, and REM sleep is absent. The dominant finding in TCI-DISE is often tongue-base collapse — a pattern consistent with the generalised muscle tone suppression of anaesthesia, which may or may not represent what happens during genuine sleep. Some patients have REM-related obstruction as their primary pathology, which TCI-DISE will miss completely. Others may have positional OSA that is invisible when the patient is immobilised on an operating table rather than free to reposition naturally.
Professor Veer developed a physiologically informed modification of DISE to address these limitations — now submitted for peer review in the Journal of Laryngology and Otology.
The Technique in Detail
The key modification is simple in principle but requires patience and a well-prepared environment. Rather than maintaining a continuous sedation level throughout the procedure, Professor Veer administers a single bolus of propofol (approximately 2 mg/kg, adjusted for body weight and comorbidity), then uses the brief period of anaesthesia to assess static anatomical features — septal deviation, turbinate hypertrophy, tonsil size, vocal cord anatomy — that are independent of sleep state.
The nasendoscope is then parked just posterior to the uvula, in a position that allows unobtrusive observation of the oropharynx and larynx. The operating environment is modified: lights dimmed, noise reduced, blood pressure monitoring paused, alarms silenced. The patient is kept warm. The team remains completely still.
Over the following 10–25 minutes, propofol redistributes from the brain to peripheral tissues before being metabolised and excreted. As the drug level falls, the patient recovers from anaesthesia — but rather than waking fully, they fall into genuine physiological sleep. DISE assessment begins only once clear features of natural sleep are present:
- Cyclical respiratory variation — progressive hypoventilation, obstruction, arousal, and post-arousal hyperventilation — reflecting intact chemoreceptor-driven respiratory control rather than anaesthetic suppression
- Features consistent with REM sleep: ocular movements visible through closed eyelids, subsequent dream recall on awakening
- Behavioural indicators: yawning, spontaneous repositioning, startle response to verbal address
Supplemental oxygen — given initially for patient safety — is withdrawn once spontaneous ventilation resumes, to avoid blunting the physiologically important hypoxic drive that drives the obstructive events being observed.
Why It Produces Better Findings
Over more than a decade of using this technique, Professor Veer has observed several consistent advantages over conventional TCI-DISE:
- Reduced tongue-base collapse: by avoiding sustained propofol-induced muscle tone suppression, tongue-base obstruction appears less frequently, suggesting the high rate of tongue-base findings in TCI-DISE may partly be an anaesthetic artefact
- REM-related obstruction is visible: some patients have their dominant obstruction during REM sleep, when muscle tone is physiologically at its lowest — TCI-DISE misses this entirely; the modified technique captures it
- Positional effects are observable: patients repositioned spontaneously during natural sleep allow real-time assessment of positional OSA; the same patient may have marked improvement in the lateral position compared to supine, information that directly guides whether positional therapy is appropriate
- Arousal patterns are informative: the cyclical pattern of obstruction and arousal observed during natural sleep endoscopy more closely reflects the pathophysiology of OSA as it occurs night after night
The technique does require more time and greater anaesthetic collaboration than TCI-DISE, and is not suitable for all patients or settings. But for complex patients — those with severe OSA, those who have failed previous surgery, or those in whom the primary obstruction is unclear — it may provide substantially more accurate surgical guidance.
The PTLTbE Classification System
Published in Sleep and Breathing (2020; 24:1685–1693), the PTLTbE classification was developed by Professor Veer together with Henry Zhang, Rishi Mandavia, and Nishchay Mehta — all based at the Royal National Throat Nose and Ear Hospital. It was presented at three international conferences during development: Sleep Congress Rimini (2016), the European Respiratory Society London (2018), and the American Academy of Otolaryngology–Head and Neck Surgery Annual Meeting in Atlanta (2018).
Why a New Classification Was Needed
The qualitative research that informed PTLTbE identified several specific problems with existing systems:
- Distinction between tonsillar and lateral wall obstruction was absent or ambiguous. Tonsillectomy and expansion sphincter pharyngoplasty are fundamentally different operations for fundamentally different structures. Any classification that conflates them — or places them in the same category as "oropharyngeal obstruction" — cannot reliably guide the choice between them.
- Percentage obstruction was unreliably estimated. Asking observers to classify obstruction as 0–25%, 25–50%, 50–75%, or greater than 75% generated extremely poor inter-rater agreement. Even experienced practitioners could not reliably differentiate anything more precisely than "more or less than 50%."
- The learning curve for existing systems was steep. Junior surgeons often identified the most obvious abnormality and missed co-existing obstructive levels — a tonsillar obstruction would be recorded, but a concurrent tongue-base collapse left undocumented.
- Classification systems varied in complexity in a way that made them useful only to specialists — a system that needed to be looked up on a reference card was rarely used consistently in day-to-day practice.
The design of PTLTbE was guided by two models of success: the TNM cancer staging system (which forces exhaustive level-by-level assessment rather than overall impression), and visual learning (which has a shorter acquisition curve than textual description for dynamic findings).
The Name: PTLTbE
The name is deliberately not elegant. It stands for Palate — Tonsil — Lateral pharyngeal wall — Tongue base — Epiglottis: the five anatomical sites assessed during DISE, in the precise order a flexible nasendoscope encounters them during a standard examination. The name forces the user to consider each level individually and in sequence, in the same way the TNM system forces the oncologist to record T, N, and M stages independently rather than giving an overall impression.
Each level is graded 0, 1, or 2:
- 0 — No obstruction; normal appearance
- 1 — Obstruction of less than 50% of the airway at that level
- 2 — Obstruction of 50% or more at that level
The exception is the Epiglottis level, which uses only 0 (normal) or 1 (abnormal), since epiglottic obstruction is either present or it is not — the various forms of epiglottic pathology (trapdoor, omega/horseshoe, laryngomalacic) do not differ materially in clinical significance.
The Five Levels — A Level-by-Level Guide
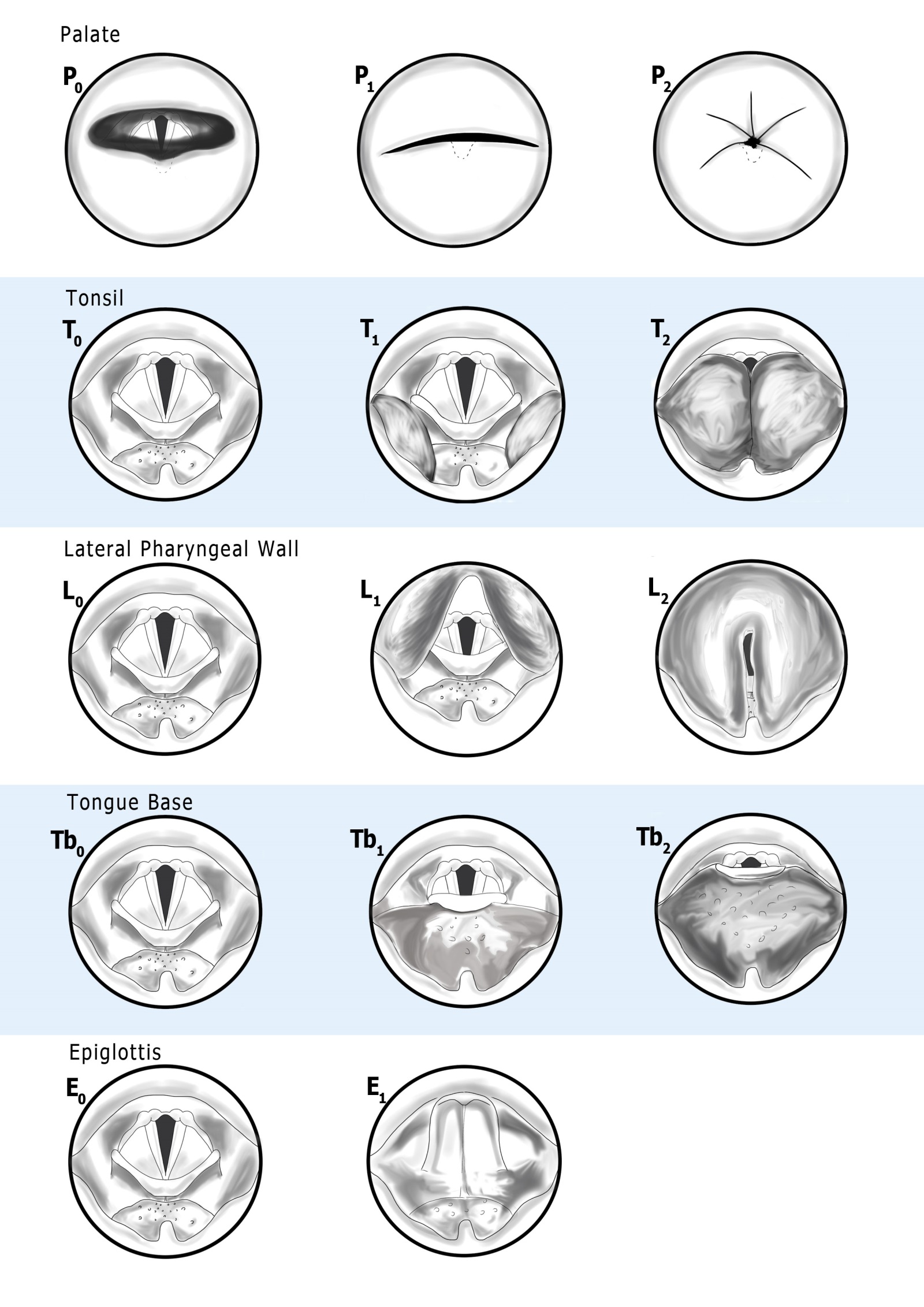
What follows is a full clinical description of each level, with the original classification images from the published paper. These images serve as the visual aide-memoire that makes the system practical to use on a daily basis without constant reference to a table.
P — The Palate Level
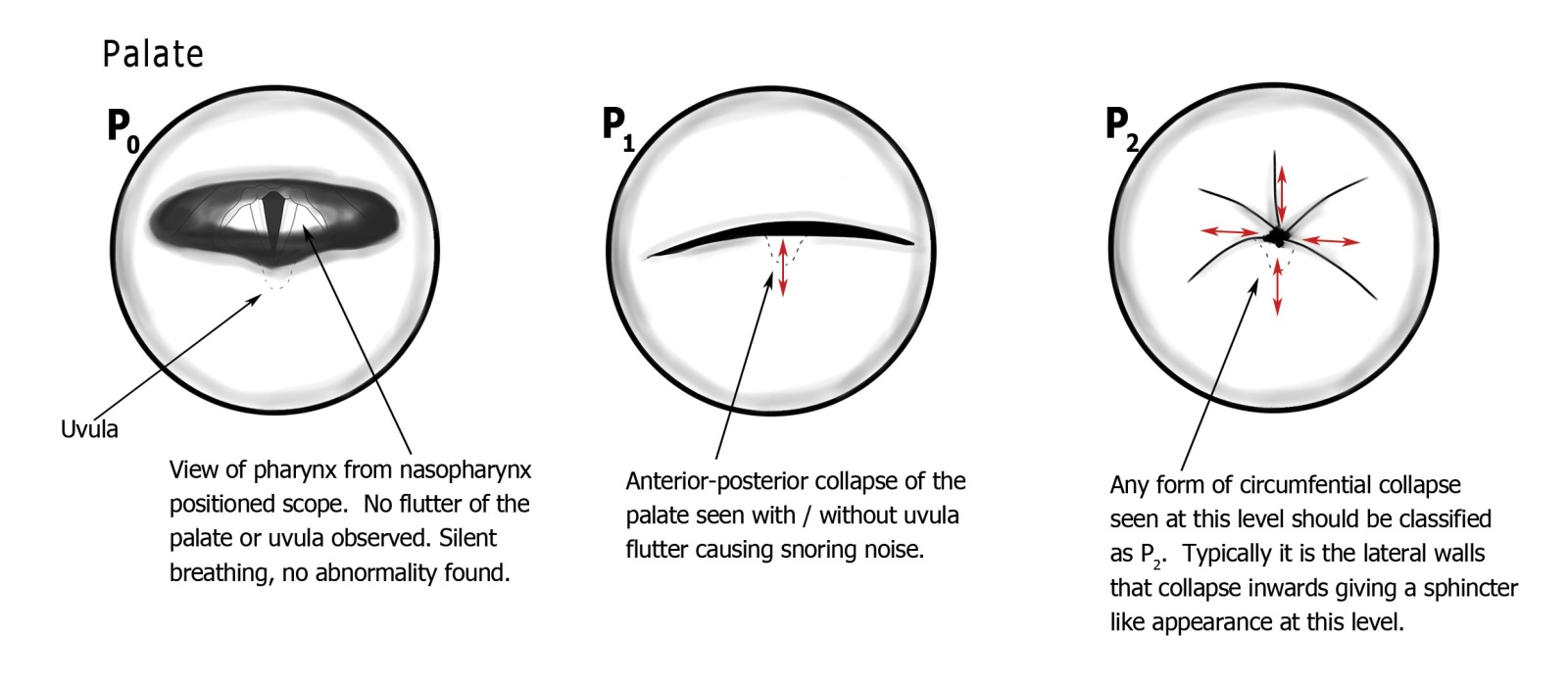
The palate is assessed from the nasopharynx — the view obtained by passing the nasendoscope through the nose and looking down and back at the soft palate and uvula from above. In individuals without sleep-disordered breathing, the palate and uvula remain relatively motionless during respiration, and the pharyngolarynx is clearly visible behind them.
Three classes are defined:
- P0 — Normal: No flutter or obstruction at the palatal level. The posterior pharynx is fully visible throughout the respiratory cycle.
- P1 — Anteroposterior (AP) collapse: The soft palate or uvula flutters or collapses anteroposteriorly, without significant lateral nasopharyngeal wall involvement. This is the most common pattern in simple snoring.
- P2 — Circumferential collapse: Both AP and lateral collapse occur, resulting in the palate and lateral walls meeting to close the nasopharynx circumferentially. This pattern is relevant as an exclusion criterion for hypoglossal nerve stimulator implantation (Inspire).
The distinction between lateral and circumferential collapse — present in some other classification systems — was deliberately removed in PTLTbE after testing showed this distinction was consistently confused by junior observers. The P1/P2 distinction (AP vs. circumferential) retained both clinical utility and adequate inter-rater reliability.
T — The Tonsil Level
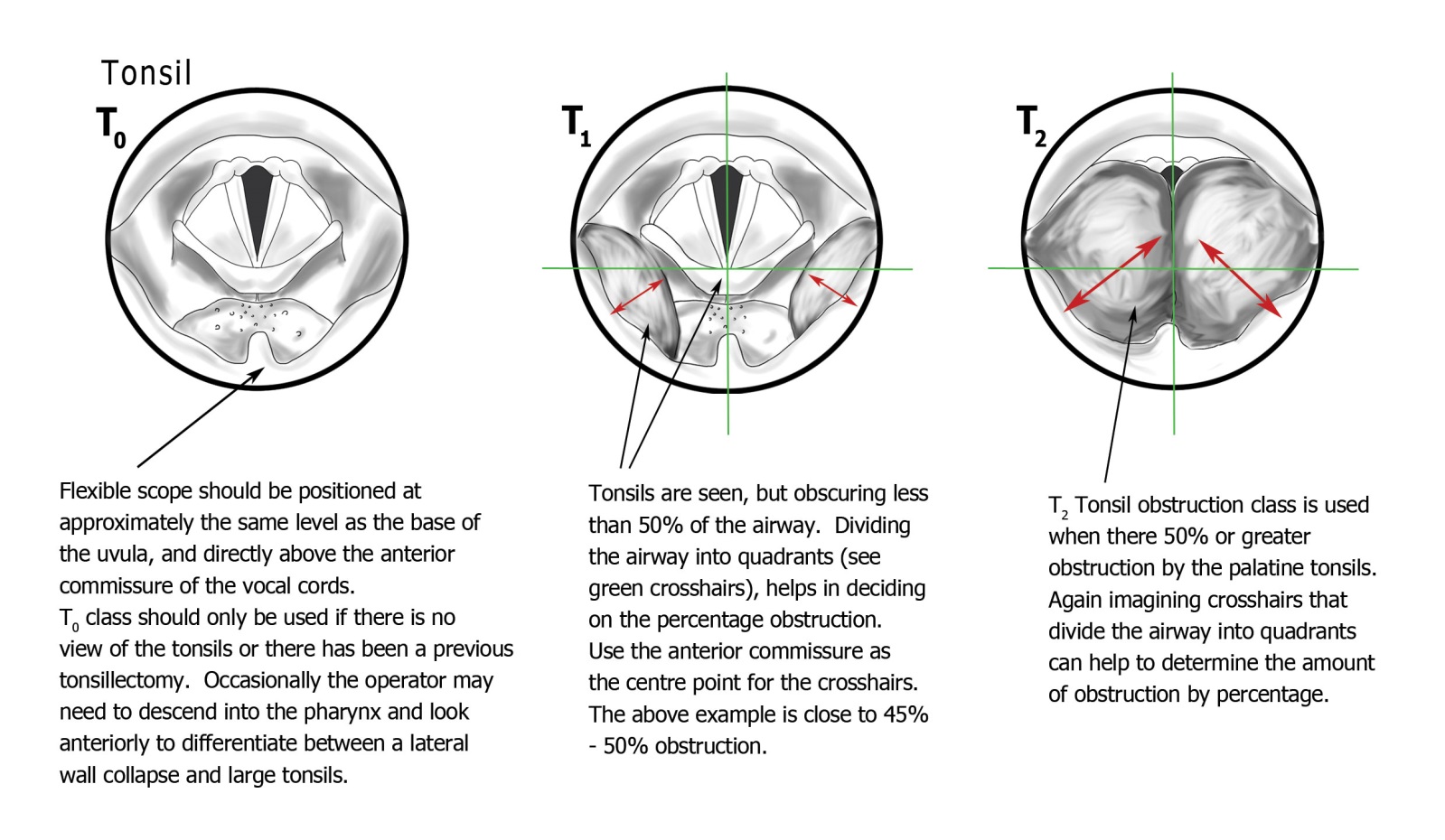
With the nasendoscope advanced to the level of the base of the uvula — positioned directly above the anterior commissure of the larynx, which serves as a consistent midpoint landmark — the palatine tonsils are assessed. The anterior commissure is deliberately chosen as the reference point because it is visible in virtually all patients and provides a reproducible midpoint from which percentage obstruction can be estimated.
To aid percentage estimation, the observer is advised to project imaginary crosshairs centred on the anterior commissure, dividing the airway into four roughly equal quadrants. Tonsillar obstruction characteristically advances from the lateral lower quadrants toward the midline. If the tonsils have crossed the midline (anterior commissure), they are classified as T2.
- T0 — Normal or absent: No palatine tonsils visible, or previous tonsillectomy, or tonsils present but not obstructing.
- T1 — Less than 50% obstruction: Tonsils encroach on the airway but have not reached the anterior commissure (midpoint).
- T2 — 50% or greater obstruction: Tonsils meet or cross the midline. Tonsillectomy is likely to be beneficial.
An important clinical point: tonsils can appear small on outpatient examination — sitting neatly in their fossae with little visible tissue — while still having a substantial pharyngeal component that is only apparent during DISE when they relax and prolapse medially. The DISE examination is therefore particularly valuable for patients whose tonsils appear unremarkable on clinical examination but whose sleep study suggests a significant obstruction.
L — The Lateral Pharyngeal Wall
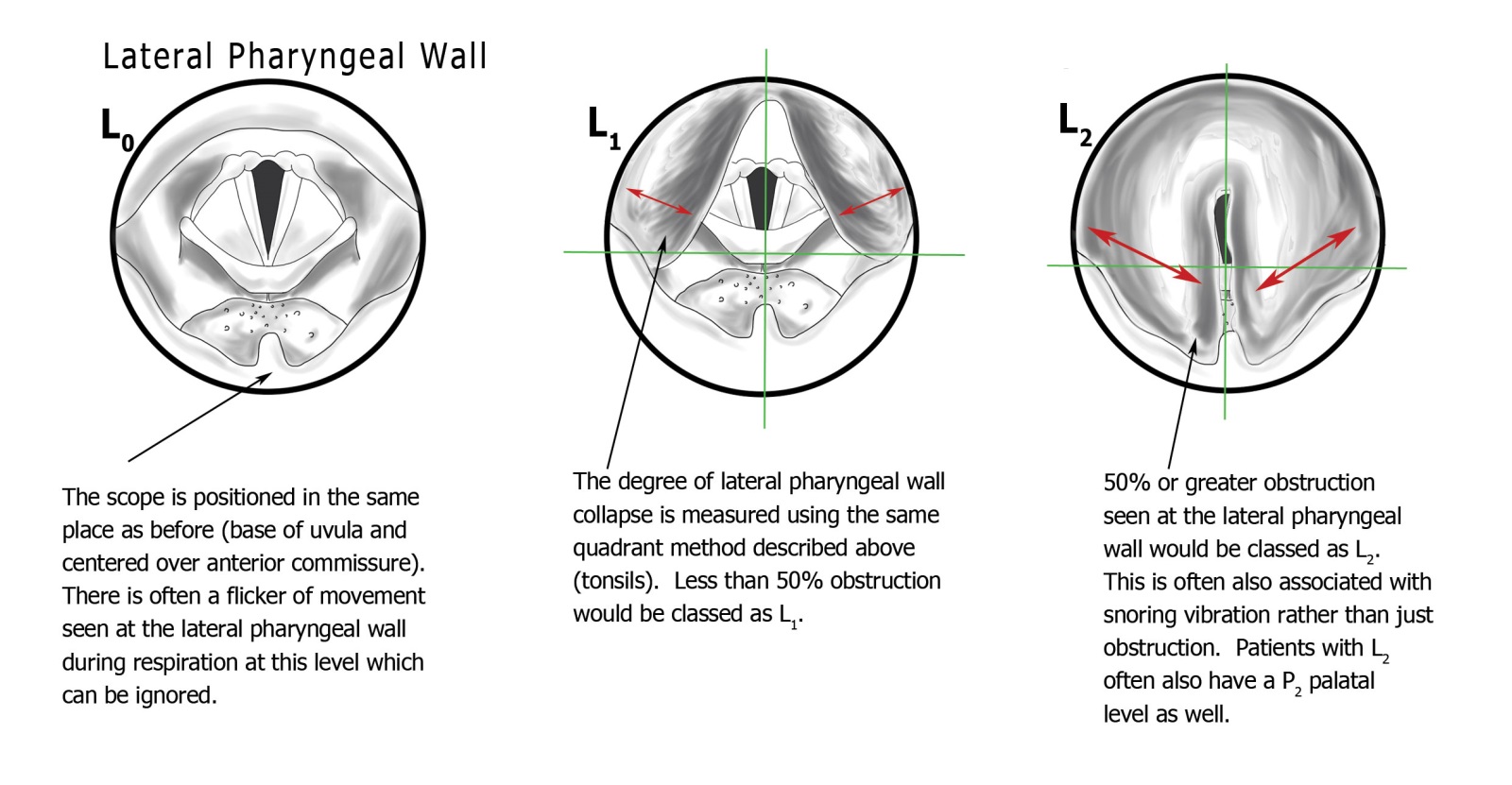
This is the level that most distinguishes PTLTbE from earlier classification systems. The lateral pharyngeal wall — the tissue visible posterior to the tonsils and posterior to the uvula, extending from the soft palate down to the level of the hyoid — is assessed at the same nasendoscope position as the tonsillar level.
Lateral pharyngeal wall collapse occurs independently of tonsillar obstruction, and the two require different surgical treatment. Lateral wall collapse that exceeds 50% of the airway (L2) is a strong indication for Expansion Sphincter Pharyngoplasty or a related lateral wall procedure. Tonsillectomy alone in a patient with significant L2 collapse and absent or small tonsils will not address the dominant obstructive pathology.
- L0 — Normal: Lateral walls are visible and stable. Minor respiratory flicker (less than approximately 5%) is a normal variant and should be disregarded.
- L1 — Less than 50% collapse: Lateral wall movement encroaches on the airway but has not reached the midline.
- L2 — 50% or greater collapse: Lateral walls meet or approach the midline. This may include cases where the walls produce a column of vibrating air at the midline — a characteristic pattern that generates snoring noise. Professor Veer has named the characteristic lateral wall tissue bulging visible in clinic "Pharyngeal Cushions" — a sign visible on outpatient examination in severe patients.
An important note on coexisting T and L classification: it is entirely valid to record both T2 and L2 in the same patient (e.g. P1 T2 L2 Tb0 E0). This does not imply 200% obstruction — it means that both the tonsils and the lateral walls are independently contributing to obstruction of 50% or more each. In practice the observer should try to judge which of the two is contributing more, but where this is genuinely unclear, recording both as grade 2 is reasonable and communicates the correct clinical message: that both tonsillectomy and lateral wall surgery are likely to be needed.
Tb — The Tongue Base
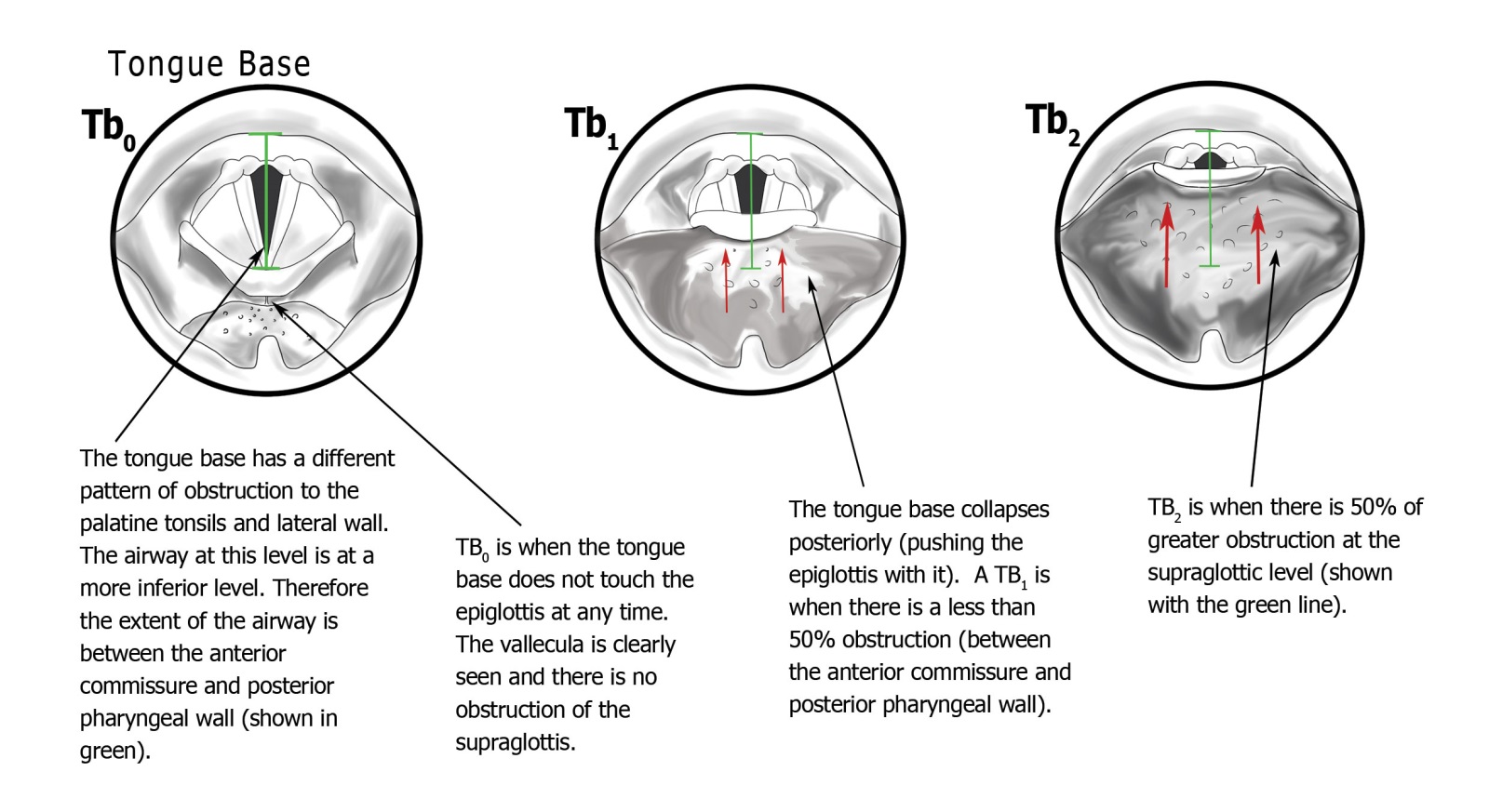
The tongue base is anatomically inferior to the palatine tonsils, occupying a different level in the pharynx. Assessment uses the same nasendoscope position as the T and L levels, but the airway geometry is different: the relevant airway at tongue base level is measured from the anterior commissure to the posterior pharyngeal wall (the posterior boundary), rather than between the lateral walls. The percentage obstruction calculation therefore uses this anteroposterior distance as the reference, with the midpoint of this line representing the 50% threshold.
- Tb0 — Normal: The tongue base does not push the epiglottis posteriorly. The vallecula is visible — this is the key landmark confirming an unobstructed tongue base level.
- Tb1 — Less than 50% obstruction: The tongue base collapses posteriorly, displacing the epiglottis and beginning to encroach on the laryngeal inlet, but does not cover more than half of the airway at this level.
- Tb2 — 50% or greater obstruction: The tongue base has collapsed to cover 50% or more of the laryngeal inlet. In calculating this percentage, the epiglottis itself is included as part of the obstructing mass — it is the laryngeal surface of the epiglottis (the surface facing the laryngeal inlet) that represents the anterior limit of the obstructed airway.
An important distinction: if the epiglottis moves posteriorly without the tongue base collapsing onto it, this is classified as an epiglottic (E) problem rather than a Tb problem. Only when the tongue base actively pushes the epiglottis back should the movement be recorded at Tb level. Where both occur independently — tongue base collapse and concurrent primary epiglottic pathology — both levels should be recorded (e.g. Tb2 E1).
Tongue base obstruction is one of the most surgically challenging findings in DISE. Options include radiofrequency ablation, coblation, robotic tongue base reduction, genioglossus advancement, and — for appropriate patients — hypoglossal nerve stimulator implantation. The choice among these is guided by the degree of collapse, the patient's anatomy, and their DISE findings at other levels.
E — The Epiglottis
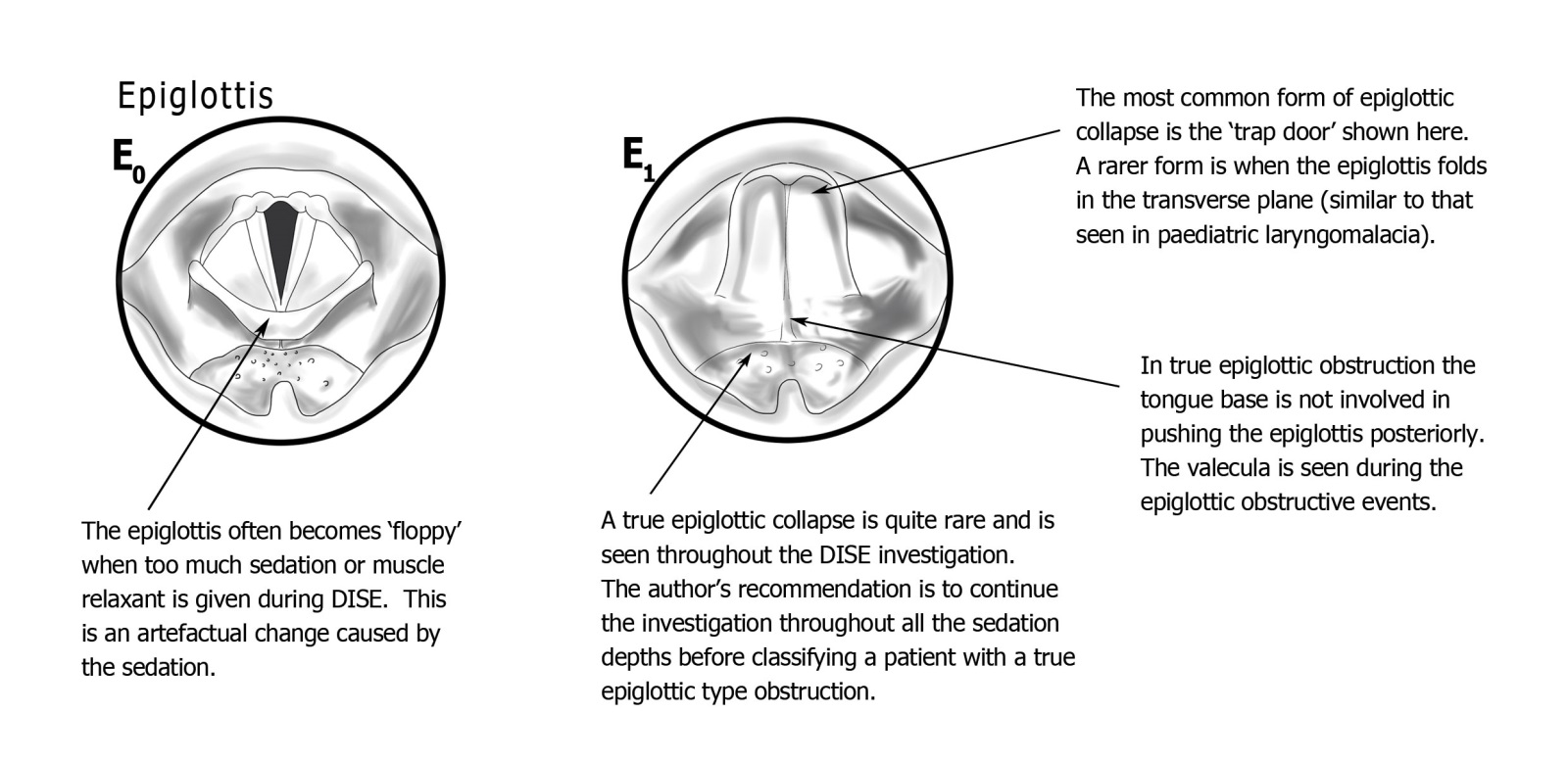
Epiglottic obstruction is less common than the other levels but clinically important, and notably underdiagnosed by investigations other than DISE. The epiglottis — designed to divert food away from the larynx during swallowing — can collapse posteriorly into the laryngeal inlet during sleep in several distinct ways:
- The trapdoor epiglottis: the most common variant. The epiglottis swings posteriorly over the laryngeal inlet with each inspiration, completely blocking airflow, then returns on expiration. This produces a characteristic regular obstruction pattern often associated with dramatic oxygen desaturations.
- The omega-shaped (horseshoe) epiglottis: an infolding of the epiglottis, similar to infant laryngomalacia, in which the lateral margins curl medially to occlude the laryngeal inlet.
- Laryngomalacic-type obstruction: indrawing of redundant arytenoid mucosa, as seen in laryngomalacia in infants, occurring in adults with severe OSA or significant negative intraluminal pressure during obstructed respiratory effort.
Because these variants differ in mechanism but not materially in severity or surgical approach, the E level uses only two classes:
- E0 — Normal: The epiglottis is not contributing to airway obstruction independently of the tongue base.
- E1 — Epiglottic obstruction: Any of the above patterns is present, representing primary epiglottic pathology rather than secondary movement from tongue base collapse.
Epiglottic Obstruction and CPAP
Epiglottic obstruction has a critical relationship with CPAP that every clinician should understand. CPAP — by increasing airway pressure — normally holds the airway open by acting as a pneumatic splint. However, in epiglottic trapdoor obstruction, the increased pressure actively forces the epiglottis further into the laryngeal inlet rather than holding it away. The result is that CPAP makes these patients worse — often dramatically so, with increasing desaturations at higher pressures.
Many patients with epiglottic obstruction are either untreated or on CPAP that is making no difference. They may have been told their sleep study is "normal" or "mild" because standard oximetry or basic polysomnography does not reliably identify the characteristic regular obstruction pattern of a trapdoor epiglottis — it may appear as a modest AHI with atypical desaturation kinetics. DISE is the only reliable way to identify it. Surgical correction — epiglottoplasty, performed as part of a multilevel surgical programme — can be highly effective.
The Complete PTLTbE Visual Guide
Figure 6 from the published paper provides the complete visual reference for all five levels simultaneously — the aide-memoire that allows the system to be used reliably after only a short learning curve.
Reading a PTLTbE Result
The final classification is written as a string of five values — one per level — expressed as subscripts. For example:
Clinical Examples
P0 T2 L0 Tb0 E0
Large tonsils meeting the midline; all other levels normal. A straightforward tonsillectomy is likely to be very effective. The surgeon can give the patient a high degree of confidence that surgery will improve their breathing.
P1 T0 L2 Tb0 E0
No tonsillar tissue but severe lateral pharyngeal wall collapse. Expansion Sphincter Pharyngoplasty is the targeted operation. A tonsillectomy (if performed without DISE) would have been pointless. Palatal work to address snoring may also be appropriate.
P2 T0 L0 Tb2 E0
Circumferential palatal collapse and significant tongue base obstruction. Multilevel disease requiring both palatal and tongue base surgery. The P2 finding also has implications for Inspire candidacy (circumferential collapse is an exclusion criterion).
P0 T0 L0 Tb0 E1
All levels normal except the epiglottis. This patient has epiglottic trapdoor obstruction as the sole finding — and may have been on CPAP that was worsening their condition. Epiglottoplasty, offered as part of Professor Veer's multilevel programme, addresses this directly.
P1 T0 L1 Tb2 E0
Palatal flutter, lateral wall involvement, and dominant tongue base collapse. Complex multilevel disease. This patient is a candidate for tongue base surgery (radiofrequency ablation, robotic reduction, or hypoglossal nerve stimulation depending on anatomy) alongside targeted lateral wall and palatal treatment.
Effect of jaw thrust:
PTLTbE allows additional notation for manoeuvres during DISE. If the example above changes to P0 T0 L0 Tb1 E0 with chin lift, and P0 T0 L0 Tb0 E0 with jaw thrust, this indicates a mandibular advancement device (MAD) would completely resolve the airway obstruction for this patient — a prediction confirmed in clinical practice.
Inter-Rater Reliability — Published Data
The practical value of any classification system rests on its ability to produce consistent results between different observers. The published validation study for PTLTbE used 20 junior doctors with no prior DISE experience, taught the classification, and then shown five DISE videos selected to represent the range of obstructive patterns. Five of the twenty were additionally taught the VOTE classification to allow direct comparison.
PTLTbE Krippendorff Alpha by Video
| Video | PTLTbE (Krippendorff α) | VOTE (Krippendorff α) | Agreement level |
|---|---|---|---|
| Video 1 | 0.86 | 0.47 | Almost perfect |
| Video 2 | 0.54 | 0.47 | Moderate |
| Video 3 | 0.82 | 0.66 | Almost perfect |
| Video 4 | 0.66 | 0.36 | Substantial |
| Video 5 | 0.71 | 0.31 | Substantial |
Landis & Koch scale: ≤0 = poor; 0.01–0.20 = slight; 0.21–0.40 = fair; 0.41–0.60 = moderate; 0.61–0.80 = substantial; 0.81–1.0 = almost perfect.
PTLTbE Percentage Agreement by Domain
| Domain | Agreement with gold standard |
|---|---|
| Palate (P) | 91.43% |
| Tonsil (T) | 97.14% |
| Lateral pharyngeal wall (L) | 86.67% |
| Tongue base (Tb) | 77.14% |
| Epiglottis (E) | 90.10% |
| Overall | 90.10% |
The lowest domain agreement was at the tongue base level (77.14%), which is consistent with the technical challenge of positioning the nasendoscope accurately when large tonsils or lateral wall collapse obstruct the view. The lateral wall level also showed lower agreement (86.67%) — reflecting the fact that lateral wall collapse is often confused with tonsillar obstruction, precisely the distinction that PTLTbE was designed to clarify. In subsequent clinical use, these challenging cases are addressed by the structured guidance in the classification images.
Compared with other published DISE classification studies: Vroegop et al. (2013) found VOTE kappa coefficients ranging from –0.03 to 0.33 in non-experienced assessors. Carrasco-Llatas et al. (2017) found VOTE kappa as low as 0.17 at the palate level between experienced and non-experienced assessors. The PTLTbE inter-rater data compares favourably to both.
How PTLTbE Guides Surgical Planning
The primary purpose of DISE — and of any classification system applied to it — is to guide the choice of operation. The PTLTbE result determines which anatomical levels require treatment, which operations are indicated at each level, and in some cases which operations are contraindicated.
P1 or P2
Palatal and uvular procedures — laser palatoplasty, radiofrequency stiffening, UPPP modifications, palatal advancement. P2 (circumferential) excludes Inspire implantation.
T2
Tonsillectomy (cold steel intracapsular technique). High confidence that tonsillectomy will be effective in absence of other levels.
L2
Expansion Sphincter Pharyngoplasty and variants, lateral wall plication. Often achieved alongside tonsillectomy (T2 L2) or independently of tonsillar tissue.
Tb2
Radiofrequency ablation, coblation, robotic tongue base reduction, genioglossus advancement, or hypoglossal nerve stimulation (Inspire / Genio). Choice depends on degree of collapse and anatomy.
E1
Epiglottoplasty, as part of a multilevel surgical programme. CPAP to be reviewed — may be worsening rather than improving obstruction in this patient.
Jaw thrust response
If PTLTbE resolves to P0 T0 L0 Tb0 E0 with jaw thrust, mandibular advancement device is predicted to be highly effective. Documented in notation alongside the standard PTLTbE result.
Professor Veer offers over 43 distinct surgical procedures, grouped across these five anatomical regions. In patients who require multiple levels of treatment, surgery is staged to allow recovery between procedures, with repeat DISE or sleep study data used to assess progress and guide the next stage. The aim is to achieve the lowest possible AHI with the least invasive combination of interventions appropriate to the individual patient's anatomy.
Publications and Conference History
Peer-Reviewed Publications
- Veer V, Zhang H, Mandavia R, Mehta N. Introducing a new classification for drug-induced sleep endoscopy (DISE): the PTLTbE system. Sleep and Breathing. 2020;24:1685–1693. doi:10.1007/s11325-020-02017-w
- Veer V, Roberts J, Lee CW. A Physiologically Informed Modification of Drug-Induced Sleep Endoscopy. Journal of Laryngology and Otology. 2025 (submitted).
International Conference Presentations
- Sleep Congress, Rimini, Italy — 2016 (first version of the PTLTbE classification)
- European Respiratory Society Annual Congress, London, UK — 2018 (draft version)
- American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Annual Meeting, Atlanta, USA — 2018 (final version)
Institutional Affiliation
All work was conducted at the Royal National Throat Nose & Ear Hospital, 330 Gray's Inn Road, London WC1X 8DA — part of University College London Hospitals NHS Foundation Trust, and the UK's leading tertiary referral centre for ENT and sleep surgery.
For Clinicians Using DISE
Professor Veer is happy to discuss the PTLTbE classification and the modified DISE technique with clinicians seeking to introduce or improve DISE in their practice. He has spoken internationally on both topics and has trained surgeons in DISE interpretation in the UK and abroad.
Key practical points for those adopting PTLTbE in their practice:
- Use the complete visual guide (Figure 6, above) as an aide-memoire during the learning phase. Most clinicians no longer need to refer to it after 10–15 DISEs.
- Always record the nasendoscope position before scoring each level. Positioning the scope too far posteriorly will artifactually improve the apparent tongue base and lateral wall findings.
- Record the effect of chin lift and jaw thrust as additional notation alongside the standard PTLTbE result — this takes 30 seconds and provides directly actionable information about MAD candidacy.
- Where tongue base and epiglottic obstruction are both present, document whether the epiglottic movement is driven by the tongue base (Tb-related) or occurring independently (E-level) — this determines whether epiglottoplasty is needed.
- For patients already on CPAP, consider whether an E1 finding explains why their CPAP is ineffective or intolerable — the counterintuitive CPAP-worsening mechanism should be explained to the patient at consultation.
- Video record all DISEs. Retrospective review frequently reveals findings missed on initial examination, particularly at the tongue base and lateral wall levels.