Blog · Sleep Science

What if back sleeping isn't normal at all — but a quirk of the modern mattress, propped up by a culture that pretends pillows have always existed?
Why this question matters
For something we spend a third of our lives doing, we ask surprisingly little about sleep posture. Most of us inherit the position our childhood beds happened to encourage, then never reconsider it. But sleep position is not a neutral choice. It changes how much air reaches your lungs, how cleanly your spine aligns, how efficiently your brain washes itself overnight, and — over decades — how well your cardiovascular and cognitive systems hold up. So it is reasonable to ask the deeper question: of all the possible postures, which one is the human body actually built for?
The honest answer, when you line up the evolutionary biology, the comparative anatomy, the airway physiology and the neuroscience, points overwhelmingly in the same direction: we are designed to sleep on our side. Not on our back. Not on our stomach. On the side, slightly curled, in something close to the recovery position.
The evolutionary clue: look at our nearest relatives
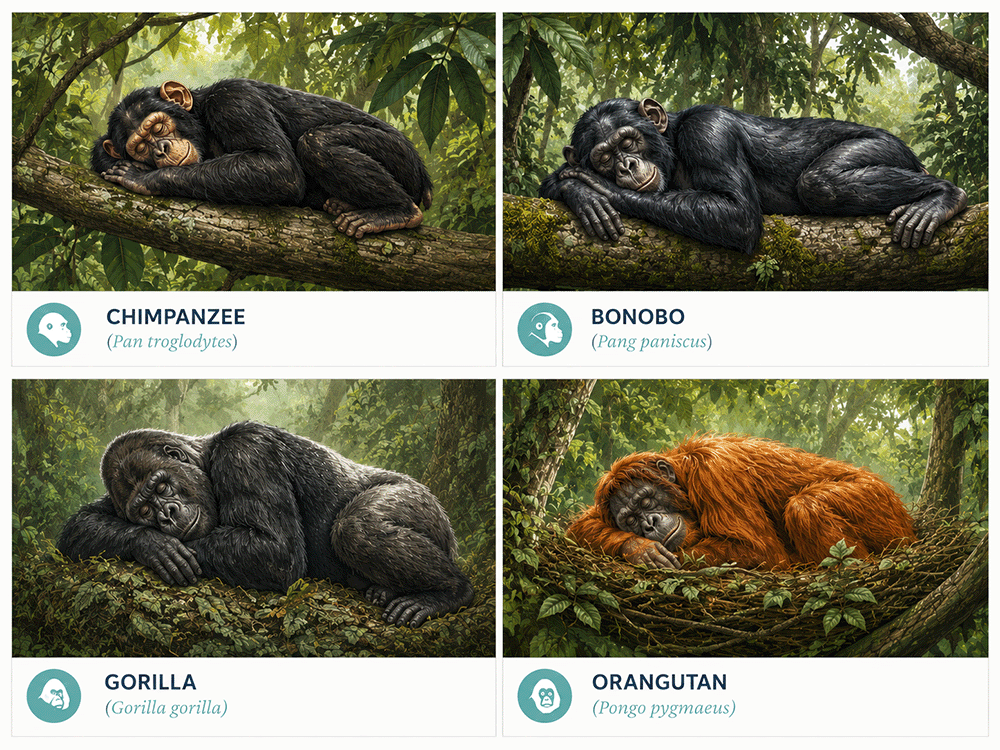
Wild great apes — chimpanzees, gorillas, orangutans, bonobos — overwhelmingly sleep on their side. Field studies of nesting behaviour describe the same posture again and again: a curled, lateral position, often with one arm cradling the head and the knees drawn up. Lying flat on the back is essentially absent from the natural primate sleep repertoire. Whatever advantage back sleeping might confer is small enough that natural selection has shrugged at it for millions of years.
This pattern is not limited to primates. Most mammals — dogs, cats, horses, elephants, cetaceans — sleep on their side or in a posture that protects the airway from gravitational collapse. The supine position is a vulnerability in the wild: it exposes the abdomen, it slows the transition to standing, and it compromises the airway. Animals that sleep on their back outside of a safe domestic environment tend not to survive long enough to pass that habit on.
Humans share the same anatomy, the same airway, and the same evolutionary heritage as these animals. There is no plausible reason that we, alone among large mammals, would be built for back sleeping.
The anatomy: the body fits the side
Stand up and look at yourself in a mirror. You are roughly the width of your shoulders. Now lie flat on the floor without a pillow. The neck must arch awkwardly because the head needs to clear the shoulders; the spine settles into a position it wasn't built for. Roll onto your side and everything realigns — head, neck and spine sit in a straight line, the shoulder finds its own pocket, and the airway opens cleanly.
The shape of the human torso confirms this. The shoulders are wider than the hips. The neck is offset above the chest. The arms rest naturally in front of the body, not at the sides. None of these features make biomechanical sense for sleeping flat on the back, but all of them work perfectly when you lie on your side with the knees drawn up and the top arm forward. The body literally has a "shoulder pocket" — the space between the shoulder and the head that demands either a pillow tall enough to fill it, or the lateral position which removes the need entirely.
The pillow is a recent invention. For most of human history we slept on the ground, or on grass, or on simple woven mats — sometimes with a wooden head rest, but never with a soft mattress beneath. The luxurious sprung mattress that lets you sleep flat on your back without pain is a 20th-century invention. The orthopaedic pillow that compensates for the gap between shoulder and head is even newer. Take both away and the human body very quickly reverts to its default position — on the side, slightly curled.
The spinal evidence reinforces this. Disc pressure studies show that supine lying does keep the spine neutral, but only on a perfectly engineered mattress; on anything firmer than a modern bed, the lumbar curve flattens uncomfortably. Side lying with a knee pillow distributes load more evenly and protects the hip-shoulder kinetic chain. Prone (stomach) sleeping forces a sustained neck rotation that no spine surgeon would ever recommend.
The brain's overnight cleaning service
Here is where the story gets interesting — and where the case for side sleeping shifts from comfort to consequence.
In 2012 a research group described the glymphatic system: a network of channels around the brain's blood vessels that flushes cerebrospinal fluid through brain tissue overnight, carrying away metabolic waste. The clearance includes amyloid-beta, the same protein that accumulates in Alzheimer's disease. Glymphatic activity is dramatically higher during sleep than wakefulness — one of the leading explanations for why long-term sleep deprivation is so neurologically damaging.
The key finding for our purposes came in 2015: in rodent models, glymphatic clearance was most efficient when the animal slept on its side. Less efficient when lying on the stomach. Least efficient on the back. The difference was substantial — roughly a quarter more amyloid-beta cleared in the lateral position than in the supine one. If this finding holds in humans — and the geometry of the brain and its drainage suggests it should — then sleeping position isn't just an airway issue. It may matter for long-term brain health.
This is the part of the science that tends to get patients' attention. It is one thing to know that side sleeping reduces snoring tonight. It is quite another to consider that the same posture may, over decades, be associated with cleaner removal of the proteins implicated in Alzheimer's disease. We do not yet have the human longitudinal trial that would settle this question conclusively. But the converging evidence — that sleep apnoea increases dementia risk, that disturbed sleep impairs glymphatic clearance, and that the lateral position optimises both airway and clearance — is hard to dismiss.
The airway argument (the part I see every day)
In my own audit of 6,044 OSA patients, 60% no longer met the clinical threshold for sleep apnoea on their side. That isn't an abstract evolutionary argument — that's measurable airway physiology. When you lie on your back, gravity pulls the tongue and palate into the airway. On your side, gravity does the opposite. The body is engineered to keep that airway open in the lateral position, and to compromise it in the supine one.
The same effect shows up in snoring intensity, in oxygen saturation, in the number of arousals per hour, and in heart-rate variability overnight. Across every measurable axis of sleep quality, the lateral position outperforms the supine. The only reason this isn't widely appreciated is that very few people have ever had their sleep formally studied in both positions on the same night.
It also explains a clinical pattern I see constantly. Many of my patients have what we call positional sleep apnoea — their disease is overwhelmingly worse on the back. For these people, training themselves to stay on the side is genuinely curative. It is the closest thing to a free intervention I can offer. No surgery, no machine, no device — just the position the body was already built for.
The heart and circulation argument
Sleep position also influences cardiovascular load. Left-side sleeping in particular is associated with reduced gastric reflux and better cardiac output in heart-failure patients. Right-side sleeping tends to be more comfortable for healthy individuals. Both lateral positions reduce the intrathoracic pressure swings caused by partial airway obstruction — which means less mechanical stress on the heart and great vessels over the course of the night.
For patients with high blood pressure, atrial fibrillation, or any condition aggravated by sympathetic ("fight-or-flight") activation overnight, the difference between back and side sleeping is not cosmetic. It is part of how their body recovers.
So why do we keep sleeping on our backs?
- Modern mattresses are soft enough to make back sleeping pain-free
- Pillows are tall enough to lift the head off the back of an over-soft mattress
- Cultural messaging — "sleep flat" advice in pregnancy, post-surgery recovery, illness
- Comfort: many people genuinely find back sleeping immediately easier
None of these are biological reasons. They are conveniences of modern life. The trouble is that the convenience comes with a measurable cost — louder snoring, more apnoeas, possibly slower brain waste clearance, and a sleep architecture that doesn't quite match what the body was built to expect.
Read further
The full article — with extra detail on the glymphatic research, ape sleep studies and spinal mechanics — lives on the I Want Great Sleep blog.
Read the full article →What to do with this
You don't need a research paper to test this — you need fourteen nights. Spend two weeks deliberately starting every night on your side, in the recovery position, with a pillow tall enough to keep your spine in a straight line. Note your snoring (or your partner's complaints about it), your morning grogginess, your daytime energy. Most people are surprised by what shifts.
If your current pillow can't comfortably support the position, that's the limiting factor — not your willingness. Two issues sabotage most people's attempts: the head pillow is too short to fill the shoulder-to-head gap, so the neck angles down and feels uncomfortable; and there is nothing physically stopping them rolling onto the back during deep sleep. Both problems are solvable. The Dual Comfort Pro addresses the first by giving you a tall side and a shorter back; the Side Sleep Pro system addresses both with a head pillow plus a body pillow that gently restrains supine rotation. The free Positional Therapy eBook walks through the protocol in detail.
Two weeks is not arbitrary. The first three or four nights of any sleep change feel worse than usual — the body resists novelty even when the novelty is biomechanically correct. By the end of week one, most people sleep through the night on their side without trying. By the end of week two, the new position is the default. After that you stop having to think about it.
One caveat
If you're pregnant, recently had spinal surgery, or have a specific medical condition that affects how you sleep, follow your obstetrician's, surgeon's or specialist's advice over anything in this article. The general public-health argument for side sleeping does not override individual medical guidance.